Stability and comfort determine whether crutch use accelerates rehabilitation or generates secondary injuries that compound the original condition. Unstable assistive devices increase fall risk—studies document that 30–40% of crutch users develop compensatory upper extremity injuries from improper device selection or fitting. Comfortable crutches reduce energy expenditure, prevent tissue damage, and maintain compliance throughout recovery periods that may span weeks to years. Short-term users recovering from acute injuries prioritize stability and cost-effectiveness, tolerating minor discomfort for 4–8 weeks. Long-term users managing chronic conditions require ergonomic optimization to prevent overuse syndromes in the shoulders, wrists, and elbows that develop from sustained loading over months or years.
What Makes a Crutch Stable?
Stability during crutch-assisted gait depends on base of support geometry, center of gravity positioning, weight distribution mechanics, tip traction coefficient, and frame rigidity under dynamic loading. Base of support expands when crutch tips position 6–8 inches lateral to the feet, creating a triangular contact pattern during stance phase that resists medio-lateral perturbations. Narrow tip placement (<4 inches lateral) reduces stability margins, while excessive width (>10 inches) demands greater shoulder abduction strength and accelerates fatigue.
Center of gravity must remain within the base of support boundaries throughout the gait cycle—deviations beyond stability margins trigger compensatory trunk lean or rapid limb adjustments that consume energy and increase fall risk. Forearm crutches position the user’s center of gravity more anteriorly compared to underarm designs, requiring greater core strength and balance for controlled ambulation. Weight distribution across bilateral crutches follows asymmetric patterns during three-point gait—the lead crutch absorbs 40–60% of bodyweight during weight acceptance, while the trailing crutch provides 20–30% during push-off. Unequal loading creates rotational moments that destabilize novice users lacking compensatory postural control.
Tip traction determines slip resistance on various surfaces—rubber compounds with Shore A durometer 65–75 provide optimal grip on tile, wood, and concrete while maintaining wear resistance. Tips smaller than 0.875 inches diameter concentrate floor stress and increase slip probability on smooth surfaces. Frame rigidity influences stability by preventing unwanted flexion during weight transfer—aluminum frames with 1-inch outer diameter tubing deflect 2–4mm under 200-pound loads, creating subtle instability that some users perceive as device failure.
What Makes a Crutch Comfortable?
Comfort arises from appropriate grip pressure distribution, neutral wrist alignment throughout the gait cycle, effective shock absorption reducing impact transmission, ergonomic cuff design preventing tissue compression, and minimal device weight reducing upper extremity fatigue.
Grip pressure concentrates on the thenar and hypothenar eminences during weight-bearing—peak pressures reach 150–250 mmHg with hard plastic grips, sufficient to compress superficial blood vessels and cause hand numbness after 15–30 minutes of continuous ambulation. Gel-padded or contoured grips distribute load across broader palmar surfaces, reducing peak pressures by 25–35% and extending comfortable ambulation time to 60–90 minutes. Cylindrical grips 1–1.25 inches diameter accommodate 90% of adult hand sizes; larger diameters cause grip fatigue in smaller hands.
Wrist alignment determines load transmission efficiency—neutral wrist position (0–10° extension) allows optimal force transfer through the radiocarpal joint without stressing ligamentous structures. Excessive wrist extension (>20°) during stance phase concentrates compressive loads on the dorsal radiocarpal joint, causing pain and accelerating osteoarthritic changes with prolonged use. Adjustable handgrip angles (available on premium models) permit individualized alignment matching natural wrist biomechanics.
Shock absorption protects upper extremity joints from repetitive impact forces generated during heel strike—unattenuated impacts reach 1.5–2.0× bodyweight and transmit through the wrist, elbow, and shoulder at rates exceeding 50 impacts per minute during normal-paced ambulation. Spring-loaded dampening systems integrated into crutch frames absorb 15–25% of impact energy, reducing cumulative joint stress. Elastomer grips provide additional vibration dampening, particularly beneficial on hard surfaces like concrete or tile. Cuff design influences forearm comfort—vinyl-coated contoured cuffs distribute compressive forces across 4–6 square inches of forearm surface area, whereas poorly designed cuffs concentrate load on bony prominences causing bruising and soft tissue irritation.
Device weight directly affects fatigue during extended ambulation—each additional 100 grams per crutch increases upper extremity metabolic demand by approximately 3–5% over 30-minute walking periods. Standard aluminum crutches weigh 2–3 pounds per pair; carbon fiber models reduce this to 1–1.5 pounds, significantly extending comfortable use duration for patients with limited upper body strength.
Types of Crutches for Adults
Forearm Crutches (Elbow Crutches)
Forearm crutches feature a forearm cuff terminating 2–3 inches below the elbow and a handgrip positioned to maintain 20–30° elbow flexion during stance phase. These designs eliminate axillary contact, distributing compressive forces across the proximal forearm and hand rather than the armpit.
Best for long-term use: Studies demonstrate that forearm crutches reduce energy expenditure by 15–20% compared to underarm designs, enabling extended daily use for months to years without developing secondary overuse injuries. Patients requiring assistive devices beyond 12 weeks show significantly fewer upper extremity complications with forearm models. Better posture: Forearm crutches promote upright trunk positioning by eliminating the forward lean common with underarm designs, reducing spinal stress and preventing compensatory back pain. The ergonomic design encourages proper shoulder positioning and discourages hunching patterns that develop with prolonged underarm crutch use.
Greater maneuverability: Compact profile and lighter weight (typically 30–40% less than equivalent underarm models) facilitate indoor navigation, stair climbing, and integration into activities of daily living including door operation and object carrying. Users report greater independence and improved quality of life compared to bulkier underarm alternatives. Wrist fatigue considerations: Peak forces at the wrist during forearm crutch ambulation reach 40–60% of bodyweight during swing phase, necessitating adequate wrist extensor strength. Patients with pre-existing carpal tunnel syndrome, wrist arthritis, or weak grip strength may experience accelerated hand fatigue requiring ergonomic grip modifications or alternative device selection.
Underarm Crutches (Axillary)
Axillary crutches position the upper support pad 1–2 inches below the axilla, providing three-point contact through both handgrips and the underarm pads. Proper technique requires weight-bearing through the hands, using shoulder girdle stabilization rather than axillary compression.
Best for short-term use: Underarm crutches prove optimal for temporary injuries healing within 8–12 weeks, offering maximum stability through three-point contact at lower cost ($20–60 versus $60–200 for forearm models). The intuitive design requires minimal gait training, with most patients achieving proficiency in 1–2 sessions. Higher energy cost: Metabolic studies document that underarm crutch ambulation consumes approximately twice the oxygen compared to normal walking, and 15–20% more than forearm crutch gait at equivalent speeds. The increased energy demand limits sustainable ambulation distance and accelerates fatigue, particularly in elderly or deconditioned patients.
Risk of nerve compression: Prolonged pressure on the axilla compresses the brachial plexus and radial nerve against the humerus, causing crutch palsy characterized by wrist drop, hand numbness, and muscle weakness. Symptoms develop when patients lean on axillary pads rather than supporting weight through handgrips—proper education prevents this complication, but compliance challenges persist with novice users.
Bariatric Models
Bariatric crutches accommodate users exceeding 300 pounds through reinforced aluminum or steel frames rated for 400–600 pounds capacity. Frame tubing diameter increases from standard 1-inch to 1.25–1.5 inches, with reinforced joints using through-bolts rather than spring-pins. Wider handgrips accommodate larger hand circumference, and heavy-duty rubber tips with broader base diameter (1.25–1.5 inches versus 0.875 inches standard) improve stability and reduce floor stress concentration. Both axillary and forearm designs offer bariatric versions, with weight capacities extending to 650 pounds for the heaviest-duty steel models.
Heavy-Duty & Reinforced Frames
Heavy-duty crutches bridge the gap between standard and bariatric models, typically rated for 300–400 pounds. These designs use thicker-wall aluminum tubing or reinforced construction at stress points (handgrip junction, adjustment collars, tip ferrules) to increase load capacity without the weight penalty of full bariatric steel frames. Suitable for patients approaching standard weight limits who prefer lighter devices, or for users who generate high dynamic loads during athletic activities or rough terrain ambulation.
| Type | Stability | Comfort | Long-Term Use | Weight Capacity | Best For |
|---|---|---|---|---|---|
| Forearm (Elbow) | Good—requires balance | Excellent—ergonomic design | Optimal—low fatigue | 250–350 lbs standard | Chronic conditions, extended recovery >12 weeks, active users |
| Underarm (Axillary) | Excellent—three-point contact | Fair—discomfort >8 weeks | Poor—nerve risk, fatigue | 250–300 lbs standard | Acute injury <12 weeks, elderly needing max stability, first-time users |
| Bariatric (Both Types) | Excellent—wider base | Good—sized for larger habitus | Condition-dependent | 400–650 lbs | Users >300 lbs, high dynamic loads, safety-critical applications |
| Heavy-Duty Reinforced | Excellent—stronger frame | Good—standard ergonomics | Moderate—depends on type | 300–400 lbs | Users 270–350 lbs, athletic activities, rough terrain |
Stability vs Comfort Trade-Off
Frame rigidity creates a fundamental tension between stability and comfort—more rigid frames provide superior stability by preventing unwanted flexion during weight transfer, but transmit greater impact forces to upper extremity joints, reducing comfort during extended use. Aluminum frames with thin walls (0.065 inches) flex 3–5mm under load, absorbing some shock but creating perceptible instability that undermines confidence. Thick-wall aluminum or steel construction eliminates flexion, maximizing stability at the cost of increased weight and higher impact transmission.
Softer grip materials (gel, memory foam, elastomer) enhance comfort by distributing pressure and absorbing vibration, but may reduce proprioceptive feedback and precise control during rapid weight shifts or uneven terrain navigation. Hard plastic grips provide maximum tactile feedback and control but cause accelerated hand fatigue and callus formation. Premium models offering interchangeable grips allow users to balance comfort and control based on activity demands.
Open cuff versus closed cuff designs present another stability-comfort trade-off—open cuffs (U-shaped or V-shaped) allow rapid entry and exit, facilitating activities requiring frequent crutch removal like sitting or bathroom use. Closed cuffs (circular or D-shaped) provide superior stability by preventing forearm escape during unexpected perturbations, but require threading the hand through the opening, complicating donning and doffing. Most long-term users prefer open cuffs for daily convenience despite the modest stability reduction.
Materials & Frame Construction
Aluminum
Aluminum alloys (6061-T6, 7075-T6) dominate modern crutch construction, producing devices weighing 2–3 pounds per pair for standard models while supporting 250–300 pound users. The favorable strength-to-weight ratio reduces upper extremity fatigue—metabolic studies show 10–15% lower energy expenditure with aluminum versus steel crutches during 30-minute ambulation trials. Adjustability through drilled holes and spring-pin mechanisms enables precise height customization in 0.5–1 inch increments. Corrosion resistance prevents rust formation in humid environments or with perspiration exposure. Aluminum costs $25–80 for standard models and $90–150 for bariatric versions.
Steel
Steel construction delivers maximum strength at lower cost ($15–50 per pair) but increases weight to 4–6 pounds per pair. The additional mass accelerates upper extremity fatigue, particularly problematic for elderly or deconditioned patients with limited shoulder strength. Steel requires powder-coating or chrome plating for corrosion protection; coating damage exposes bare metal to rust. The material stiffness provides rigid stability preferred by heavier users who require uncompromising structural integrity. Steel dominates bariatric applications where frame strength outweighs weight considerations—models rated for 500–650 pounds typically use steel construction.
Carbon Fiber
High-modulus carbon fiber composite achieves exceptional strength-to-weight ratios, producing crutches weighing 1–1.5 pounds per pair (27% of comparable commercial aluminum devices) while maintaining 300+ pound capacity. Manufacturing complexity increases cost to $200–400 per pair, limiting adoption to long-term users prioritizing performance, elite athletes, or patients with severe upper body weakness requiring minimum device weight. Carbon fiber demonstrates excellent fatigue resistance, maintaining structural integrity through millions of loading cycles without stress-crack formation that develops in aluminum after 2–3 years of daily use. Catastrophic failure risk from impact damage (dropping, striking objects) remains a concern—carbon frames crack without visible warning signs unlike aluminum’s deformation patterns.
| Material | Weight (per pair) | Durability | Flex Characteristics | Shock Transfer | Cost Range | Best Application |
|---|---|---|---|---|---|---|
| Aluminum | 2–3 lbs | Good—2–3 years daily | Moderate flex—some absorption | Moderate | $25–150 | General use, adjustability needed |
| Steel | 4–6 lbs | Excellent—5+ years | Minimal flex—rigid | High | $15–60 | Bariatric, budget-conscious, durability priority |
| Carbon Fiber | 1–1.5 lbs | Excellent—5+ years | Minimal flex—very rigid | Low—excellent dampening | $200–400 | Long-term use, weight-sensitive users, performance |
Weight Capacity & Adult Considerations
Standard crutches accommodate 250–300 pounds, representing the 5th to 85th percentile of adult male weight distribution and 5th to 95th percentile for adult females. These specifications include safety factors of 1.5–2.0×, meaning frames undergo failure testing at 375–600 pounds. However, dynamic loading during stairs, rapid gait, or uneven terrain generates forces 1.5–2.0× static bodyweight, effectively reducing practical capacity. A 250-pound user ascending stairs may generate 375–500 pounds peak force, approaching or exceeding safety margins on standard 300-pound rated devices.
Bariatric ranges span 400–600 pounds to accommodate users exceeding standard limits with appropriate safety margins. These devices use reinforced construction—thicker tubing walls, larger diameter frames, through-bolt adjustments replacing spring-pins, and oversized rubber tips distributing ground forces across greater surface area. Patients within 50 pounds of any capacity rating should upgrade to the next weight class to preserve structural safety margins accounting for dynamic loads and weight fluctuations.
Adult considerations extend beyond simple weight capacity—taller individuals (>6’2″) require extended-length models with adjustment ranges reaching 60–64 inches to achieve proper axillary clearance and elbow angle. Shorter adults (<5’2″) benefit from compact models preventing excessive weight and facilitating easier maneuverability. Hand size influences grip diameter selection—men typically require 1.125–1.25 inch grips; women prefer 1.0–1.125 inches.
| Body Weight | Recommended Category | Frame Type | Safety Margin | Typical Construction |
|---|---|---|---|---|
| <220 lbs | Standard (250 lb rated) | Aluminum | 30+ lbs | Thin-wall tubing, spring-pins |
| 220–270 lbs | Standard (300 lb rated) | Aluminum or Steel | 30+ lbs | Standard wall tubing, reinforced joints |
| 270–350 lbs | Heavy-Duty (400 lb rated) | Reinforced aluminum | 50+ lbs | Thick-wall tubing, through-bolts |
| 350–500 lbs | Bariatric (500–600 lb rated) | Steel or thick aluminum | 100+ lbs | Large diameter tubing, reinforced construction |
| >500 lbs | Walker recommended | N/A—crutches marginal | N/A | Four-point support safer |
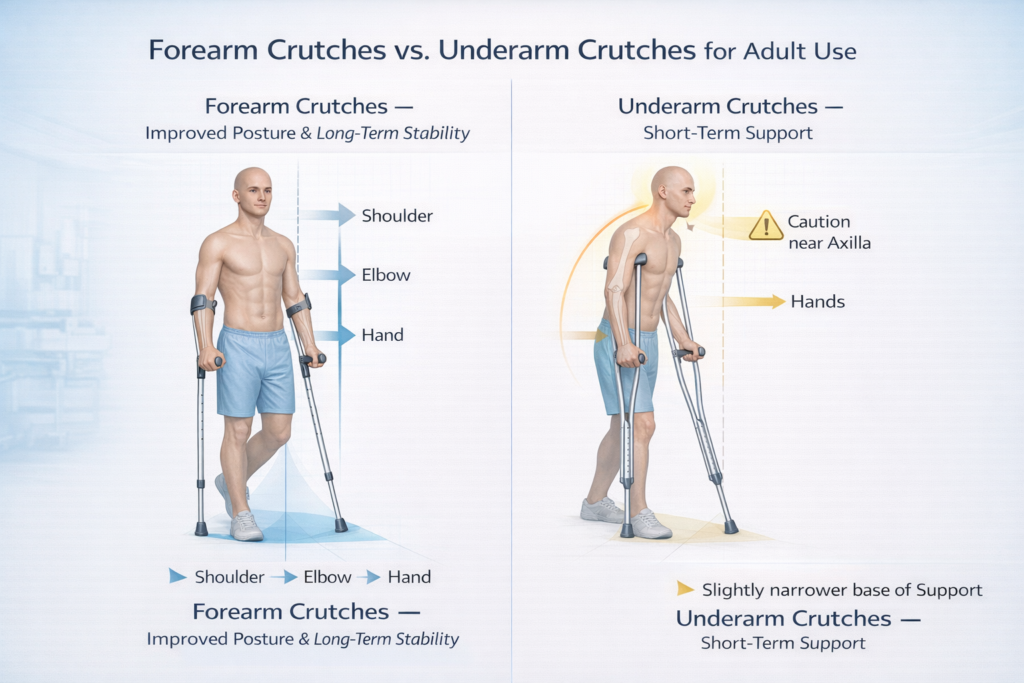
Forearm Crutches vs Underarm Crutches — Adult Comparison
Long-Term Use — What Adults Should Know
Shoulder fatigue develops from repetitive upper extremity loading during crutch-assisted gait—the anterior deltoid, rotator cuff, and trapezius muscles sustain near-continuous activation throughout stance and swing phases. Long-term users accumulate 2,000–4,000 shoulder loading cycles per kilometer of ambulation. After 3–6 months of daily use, 40–60% of crutch users report shoulder pain or weakness. Proper technique emphasizing triceps push-off rather than shoulder elevation reduces deltoid stress. Strengthening programs targeting scapular stabilizers (rhomboids, serratus anterior) and rotator cuff muscles improve endurance and reduce injury risk.
Wrist strain manifests as radiocarpal joint pain, dorsal wrist capsule inflammation, or median nerve compression symptoms after 6–12 weeks of sustained use. Peak wrist loads reach 40–60% bodyweight during weight acceptance, generating compressive forces of 100–180 pounds in a 200-pound user. Neutral wrist positioning (0–10° extension) optimizes load distribution; excessive extension (>20°) concentrates stress on dorsal joint structures. Wrist bracing during initial adaptation periods supports proper alignment while periarticular tissues strengthen. Ergonomic grips with adjustable angles allow individualized positioning matching natural wrist biomechanics.
Muscle adaptation occurs over 4–8 weeks as upper extremity muscles hypertrophy in response to sustained loading. Triceps cross-sectional area increases 8–15%, wrist extensors strengthen 12–20%, and anterior deltoid endurance improves 20–30%. This adaptation explains why initial fatigue decreases substantially after the first month of use. However, inadequate rest periods between ambulation sessions prevent adaptive recovery, leading to overuse tendinopathy rather than strength gains.
Overuse injuries affect 30–40% of long-term crutch users, including lateral epicondylitis (elbow), De Quervain’s tenosynovitis (wrist/thumb), rotator cuff tendinopathy (shoulder), and axillary soft tissue damage. Prevention strategies include proper sizing ensuring neutral joint alignment, progressive loading allowing tissue adaptation, ergonomic accessories (padded grips, shock absorbers) reducing peak stresses, strengthening exercises targeting vulnerable muscle groups, and periodic gait analysis correcting compensatory movement patterns. Switching between forearm and underarm designs distributes loading across different tissue structures, preventing chronic overload of specific anatomical sites.
Common Mistakes Adults Make
Choosing by price alone: Economy crutches ($15–25) utilize thin-wall aluminum, plastic adjustment collars prone to mechanical failure, and non-replaceable components requiring complete device replacement when parts wear. The $10–20 savings proves false economy when devices require replacement after 2–3 months versus 12–18 months for mid-tier models. Adults expecting recovery periods exceeding 8 weeks should invest in quality devices with replaceable tips, serviceable grips, and robust adjustment mechanisms.
Ignoring weight limits: Patients approaching or exceeding standard 250–300 pound capacity frequently purchase inadequate devices, unaware that dynamic loading during stairs or rapid gait generates forces 1.5–2.0× bodyweight. A 280-pound user may generate 420–560 pounds during stair descent, exceeding the safety margin of 300-pound rated crutches. Frame failure occurs suddenly and catastrophically, causing falls potentially more injurious than the original condition. Adults should select devices rated 50+ pounds above current bodyweight to preserve safety margins.
Wrong height: Self-fitting without clinical verification results in devices 2–4 inches incorrect 60–70% of the time. Crutches set too tall force shoulder elevation and lateral trunk lean; excessively short devices cause forward spinal flexion and neck strain. Both errors accelerate secondary pain syndromes and reduce stability. Professional fitting takes 15–30 minutes but prevents months of complications from improper biomechanics.
Using one crutch incorrectly: Single crutch users frequently position the device on the injured side, directly loading the healing structure rather than offloading it. Correct single-crutch technique places the device contralateral to the affected limb, reducing load on the injured side by 30–40%. Additionally, many users attempt single-crutch ambulation before achieving adequate balance (10+ second single-leg stance) or strength (ability to support 50% bodyweight per arm), increasing fall risk substantially.
When Crutches Are Not the Best Option
Severe balance deficits preclude safe crutch use—patients unable to maintain 5-second single-leg stance with eyes open lack the postural control required for the dynamic balance demands of crutch-assisted gait. Cerebellar ataxia, acute vestibular disorders, advanced Parkinson’s disease, or stroke with significant proprioceptive loss require wider-base assistive devices. Walker: Four-point contact walkers provide continuous stability without requiring dynamic balance, distributing weight across both arms and reducing strength demands per limb to 25–30% of crutch requirements. Ambulation speed decreases to 40–60% of crutch pace, and stair navigation becomes difficult, but fall risk reduces substantially for balance-impaired patients.
Upper body weakness from rotator cuff pathology, bilateral shoulder arthroplasty, or neurological conditions causing arm weakness contraindicates crutch use. Patients unable to perform five wall push-ups or support 50% bodyweight through one arm lack sufficient strength for safe ambulation. Knee scooter: Wheeled knee platforms support the affected limb in flexion while the patient propels with the unaffected leg, eliminating upper extremity loading entirely. Optimal for non-weight-bearing protocols in patients with upper body limitations, though confined to level surfaces and indoor environments.
Wheelchair: Manual or powered wheelchairs suit patients with bilateral lower extremity involvement, severe cardiovascular limitations preventing exertional activity, or temporary conditions requiring complete non-weight-bearing for extended periods (>8 weeks). Energy cost decreases to near-resting levels, but functional independence and bone density preservation suffer without regular weight-bearing activity.
Quick Selection Guide
Duration of expected use:
- <8 weeks → Underarm crutches (cost-effective, adequate for short-term)
- 8–12 weeks → Either type (personal preference and comfort)
- 12 weeks → Forearm crutches (ergonomic benefits prevent long-term injury)
User bodyweight:
- <250 lbs → Standard aluminum crutches (either type)
- 250–300 lbs → Standard heavy-duty or upgrade to 400 lb rated
- 300–400 lbs → Heavy-duty bariatric models (reinforced aluminum or steel)
- 400–500 lbs → Bariatric steel crutches (500–600 lb capacity)
- 500 lbs → Walker or wheeled device (crutches marginal for safety)
Balance and coordination status:
- Good balance (10+ second single-leg stance) → Forearm or underarm based on duration
- Moderate balance (5–10 second stance) → Underarm crutches for maximum stability
- Poor balance (<5 second stance) → Walker recommended; crutches unsafe
Upper body strength:
- Strong (can perform 10+ push-ups) → Any crutch type suitable
- Moderate (5–10 push-ups) → Underarm for short-term; forearm with ergonomic grips for long-term
- Weak (<5 push-ups) → Walker or knee scooter; crutches marginal
Primary use environment:
- Indoor only → Forearm crutches (maneuverability advantage)
- Indoor/outdoor mixed → Either type; consider shock absorption for concrete
- Stairs frequently → Underarm for maximum stability or forearm with training
- Rough terrain → Underarm crutches with oversized tips
Medical condition:
- Ankle/foot injury, short recovery → Underarm crutches
- Post-surgical lower extremity → Underarm initially; transition to forearm if >12 weeks
- Neurological condition, permanent deficit → Forearm crutches (long-term ergonomics)
- Bilateral involvement → Walker likely more appropriate
Frequently Asked Questions
Which crutches are most comfortable?
Forearm crutches provide superior comfort for use exceeding 12 weeks due to ergonomic design eliminating axillary pressure, reduced energy expenditure (15–20% less oxygen consumption versus underarm designs), and promotion of upright posture minimizing spinal stress. Within forearm designs, models featuring shock-absorbing mechanisms (spring-loaded or elastomer dampening systems), contoured gel grips distributing palm pressure across broader surface area, and adjustable handgrip angles matching natural wrist biomechanics offer maximum comfort. For short-term use under 8 weeks, properly fitted underarm crutches with thick vinyl axillary pads and cushioned handgrips provide adequate comfort without the learning curve required for forearm models. Device weight significantly impacts comfort—carbon fiber crutches weighing 1–1.5 pounds per pair reduce upper extremity fatigue by 30–40% compared to 4–6 pound steel models during extended ambulation, though cost increases substantially ($200–400 versus $15–60).
Are forearm crutches better for adults?
Forearm crutches prove superior for adults requiring assistive devices beyond 12 weeks, offering 15–20% reduced energy expenditure, better posture maintenance, lower risk of nerve compression injuries, and greater integration into activities of daily living. Medical professionals and rehabilitation specialists consistently recommend forearm designs for long-term users due to ergonomic advantages preventing secondary overuse injuries that affect 30–40% of extended underarm crutch users. However, underarm crutches remain preferable for short-term recovery (4–8 weeks) from acute injuries in adults with limited balance or upper body strength, providing maximum stability through three-point contact and requiring minimal training. Elderly adults or those with significant coordination deficits benefit from underarm stability despite comfort limitations. The optimal choice depends on expected duration, user strength and balance capabilities, and willingness to invest time mastering forearm technique requiring 2–5 training sessions versus 1–2 for underarm designs.
How do I make crutches less uncomfortable?
Reducing crutch discomfort requires addressing contact pressure points, shock transmission, device weight, and biomechanical alignment. Install gel-padded or memory foam grip covers distributing palm pressure across broader surface area and reducing peak pressures by 25–35%—these accessories cost $10–25 and extend comfortable ambulation time from 15–30 minutes to 60–90 minutes with standard grips. For underarm crutches, add thick vinyl or sheepskin covers to axillary pads preventing tissue compression and skin irritation; ensure weight transfers through handgrips rather than armpits to avoid nerve damage. Verify proper height adjustment—axillary pads should sit 2 inches below armpits with elbows bent 20–30° during weight-bearing; incorrect height causes compensatory postures generating shoulder, neck, and back pain. Replace worn rubber tips every 3–6 months when tread depth falls below 1/8 inch, as degraded tips increase impact transmission to upper extremities. Consider shock-absorbing crutch models featuring spring-loaded or elastomer dampening systems reducing impact forces by 15–25%. Strengthen upper body muscles through progressive resistance training targeting triceps, anterior deltoids, and wrist extensors—improved strength and endurance substantially reduce fatigue-related discomfort after 4–6 weeks of consistent exercise.
What is better than crutches?
No single assistive device surpasses crutches universally—optimal choice depends on specific injury characteristics, weight-bearing restrictions, user strength and balance, and functional goals. Knee scooters eliminate upper extremity loading entirely, proving superior for patients with shoulder weakness, bilateral arm injuries, or those facing extended non-weight-bearing protocols (8–12 weeks), though they perform poorly on stairs and uneven terrain. Four-point walkers provide continuous stability superior to crutches for patients with balance deficits, bilateral lower extremity involvement, or insufficient upper body strength, but limit ambulation speed to 40–60% of crutch pace and complicate stair navigation. Hands-free crutches attaching to the lower leg allow upper extremity freedom for daily activities and demonstrate 20–30% lower energy cost compared to conventional designs, though limited availability and higher cost ($300–500) restrict adoption. For specific applications, alternative devices excel: knee scooters for forefoot/ankle injuries, walkers for elderly with balance concerns, and hands-free crutches for younger active patients prioritizing independence. However, for the majority of unilateral lower extremity injuries in adults with adequate strength and balance, properly selected and fitted conventional crutches remain the optimal balance of cost, function, and recovery support.
Can I use one crutch instead of two?
Single crutch use becomes appropriate when weight-bearing status advances to partial weight-bearing (50% or greater load on affected limb), balance capacity allows 10+ second single-leg stance with eyes open, and upper body strength supports 40–60% bodyweight through one arm. Position the single crutch on the side opposite the injured limb—this contralateral placement reduces load on the affected leg by 30–40% while maintaining stable three-point gait pattern. Using the crutch on the same side as the injury provides minimal offloading benefit and creates asymmetric gait mechanics accelerating hip and back strain. Premature transition to single-crutch ambulation before achieving adequate strength and balance substantially increases fall risk and may overload healing structures causing re-injury or delayed recovery. Physical therapy evaluation should confirm readiness through specific testing: ability to ascend/descend four stairs without assistive device while holding rails, demonstration of proper single-crutch gait without Trendelenburg pattern or trunk lean, and pain-free partial weight-bearing at target percentage for 30+ minutes. Most patients progress to single-crutch use 4–8 weeks into recovery, eventually advancing to cane or unassisted ambulation as healing completes.
How do I know if crutches are stable enough?
Crutch stability adequacy manifests through confidence during weight transfer, absence of frame flexion or adjustment slippage under load, secure rubber tip traction without slipping on typical surfaces, and ability to maintain upright posture without excessive trunk lean or compensatory movements. Test stability by applying full bodyweight through both crutches while stationary—frames should not flex noticeably (>5mm deflection suggests inadequate rigidity), adjustment mechanisms should not slip or creek, and tips should grip firmly without sliding on tile or smooth surfaces. During ambulation, stable crutches allow smooth weight transfer during stance phase without wobbling, permit controlled swing-through without frame vibration, and inspire confidence ascending/descending stairs without hesitation. Instability signs include frame flexion creating bouncing sensation during weight-bearing, adjustment collar slippage causing height changes mid-use, tip slipping on smooth floors especially during lateral movements, and reluctance to trust device with full bodyweight. Verify weight capacity rating exceeds your bodyweight by 50+ pounds to preserve safety margins during dynamic loading. Check that rubber tips show adequate tread depth (>1/8 inch) and lack cracks or hardening—worn tips compromise traction significantly. If persistent instability concerns exist despite proper fitting and technique, consult physical therapist for gait analysis identifying biomechanical issues or consider upgrading to higher-quality device with reinforced construction and superior materials.