Carpal tunnel syndrome (CTS) is the most common peripheral nerve entrapment, caused by median nerve compression at the wrist within the carpal tunnel. Symptoms typically begin with intermittent hand numbness at night and progress to constant paresthesia, loss of dexterity, and thenar muscle atrophy if untreated. This guide integrates patient-level explanations with clinician-grade detail on anatomy, biomechanics, diagnosis, differential diagnosis, and both non-surgical and surgical treatment.
1. What Is Carpal Tunnel Syndrome?
Definition
Carpal tunnel syndrome is a compressive neuropathy of the median nerve as it passes through the rigid osteofibrous canal at the wrist (the carpal tunnel). The condition produces numbness, tingling, pain, and weakness in the median-innervated digits (thumb, index, middle, and radial half of the ring finger).
Clinically, CTS accounts for roughly 90% of all entrapment neuropathies, with prevalence estimates of 3–5% in the general population and higher in certain worker groups.
Anatomy of the Carpal Tunnel
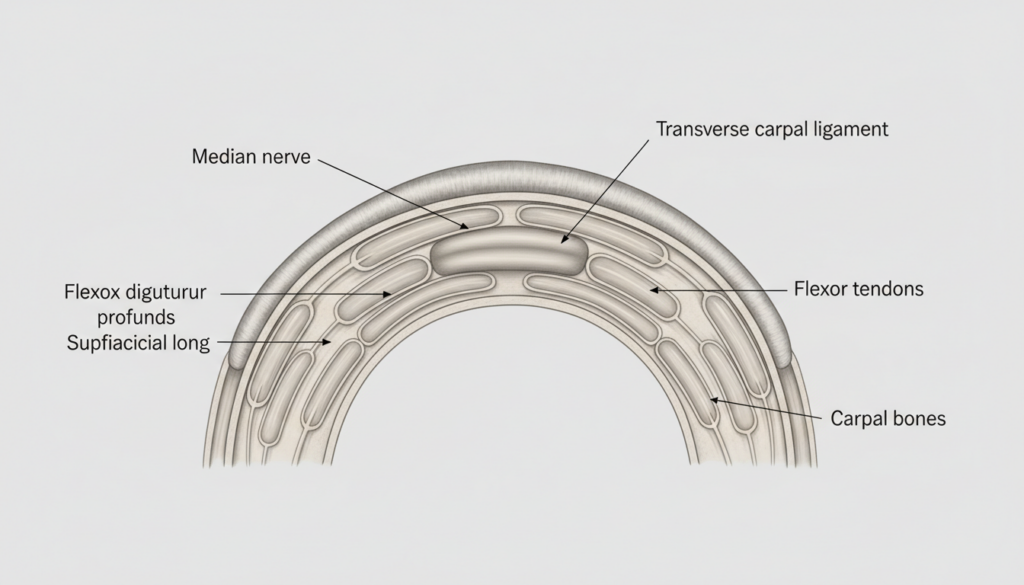
The carpal tunnel is a narrow passageway on the palmar side of the wrist formed by:
- Floor and walls (osseous): Carpal bones arranged in a concave arch.
- Roof (fibrous): Transverse carpal ligament (flexor retinaculum).
Contents:
- Median nerve
- Nine flexor tendons:
- Four flexor digitorum superficialis
- Four flexor digitorum profundus
- One flexor pollicis longus
The tunnel has limited capacity to expand; any increase in volume (synovial hypertrophy, edema, mass lesion) or reduction in canal size (fracture, deformity) increases intracarpal pressure and can trigger tunnel syndrome.
Median Nerve Function
The median nerve within the carpal tunnel:
- Sensory:
- Palmar aspect of thumb, index, middle, and radial half of ring finger
- Dorsal distal phalanges of these digits
- Motor:
- Thenar muscles: abductor pollicis brevis, opponens pollicis, superficial head of flexor pollicis brevis
- First and second lumbricals
Importantly, the palmar cutaneous branch of the median nerve arises proximal to the tunnel and travels superficial to the ligament, so the central palm often remains sensate even in advanced CTS.
Why Compression Occurs
Median nerve compression results from a mismatch between:
- Tunnel capacity: Fixed osteofibrous canal
- Tunnel contents: Tendons, synovium, median nerve
Mechanisms include:
- Increased contents volume (synovial hypertrophy, edema, hemorrhage)
- Decreased tunnel volume (post-traumatic deformity, arthritic changes)
- Dynamic changes with wrist position (extremes of flexion/extension markedly raise tunnel pressure)
Common contributing contexts:
- Systemic conditions (diabetes, hypothyroidism, rheumatoid arthritis, pregnancy)
- Occupational repetitive strain injury with high force and repetition
- Obesity and possible genetic predisposition influencing tunnel dimensions
2. Anatomy and Pathophysiology (Deep Medical Section)
Carpal Bones and Flexor Retinaculum
The carpal arch consists of:
- Radial side: Scaphoid tubercle, trapezium
- Ulnar side: Pisiform, hook of hamate
The flexor retinaculum spans these bony prominences, forming a rigid roof. Its thickness and stiffness limit expandability; increased pressure is transmitted directly to the median nerve.
The subsynovial connective tissue (SSCT) surrounds the flexor tendons and is richly vascularized and innervated. In idiopathic CTS, SSCT thickening and fibrosis are consistent pathological findings.
Pressure Dynamics Inside the Tunnel
Intracarpal canal pressure in asymptomatic individuals:
- Neutral wrist: ~2–10 mmHg
- Wrist flexion/extension: Often >30 mmHg, sometimes >90 mmHg with combined finger flexion and wrist deviation
In CTS, baseline pressures are higher and rise disproportionately with motion, driven by:
- SSCT hypertrophy and fibrosis
- Synovial proliferation and edema
- Bulging of the flexor retinaculum
- Reduced compliance of the canal
Sustained pressure >20–30 mmHg impairs intraneural blood flow, setting up ischemic neuropathy.
Ischemia and Demyelination
Pathophysiologic cascade of median nerve compression:
- Microvascular compromise
- Segmental demyelination
- Persistent or severe compression
In most CTS patients, pathology is initially demyelinating (Sunderland grade I neuropraxia); with chronic untreated compression, it progresses to axonotmesis with incomplete recovery despite decompression.
Chronic Compression Effects
Chronic CTS leads to:
- Intraneural fibrosis and thickened perineurium
- SSCT fibrosis with decreased tendon gliding and increased frictional load
- Thenar muscle atrophy from prolonged denervation
- Central sensitization and pain amplification in some patients (partly explaining symptom–test discordance)
Histologic studies show thickened SSCT with disorganized collagen, vascular proliferation, and features of chronic ischemia-reperfusion injury.
Why Symptoms Worsen at Night
Several converging mechanisms explain hand numbness at night:
- Wrist position during sleep: Many people sleep with flexed wrists, sharply increasing intracarpal pressure and median nerve compression.
- Reduced systemic blood pressure: Lower nocturnal perfusion reduces median nerve tolerance to elevated local pressure.
- Fluid redistribution: Recumbency increases fluid in the upper extremity, further narrowing the tunnel in susceptible individuals.
Clinically, nocturnal intermittent paresthesia relieved by “shaking out” the hand is highly characteristic of carpal tunnel syndrome.
3. Symptoms of Carpal Tunnel Syndrome
Early Symptoms
- Intermittent tingling or “pins and needles” in the thumb, index, middle, and radial half of the ring finger
- Hand numbness at night, often waking the patient from sleep
- Symptoms precipitated by:
Pain may radiate into the volar forearm. Symptoms usually abate with shaking or changing wrist position.
Progressive Symptoms
With ongoing median nerve compression:
- Paresthesia becomes more frequent, including daytime
- Sensory loss (reduced light touch, two-point discrimination)
- Clumsiness, dropping objects, difficulty with fine tasks (buttoning, fastening jewelry)
- Aching pain at the wrist or palm, sometimes radiating proximally
Severe Stage Symptoms
Advanced CTS is characterized by:
- Constant numbness in median digit distribution
- Markedly reduced or absent sensibility on examination
- Motor involvement:
- Thenar muscle atrophy (thenar eminence flattening)
- Weak thumb abduction and opposition
- Loss of precision grip and pinch strength
- Sometimes neuropathic pain or allodynia
At this stage, nerve damage may be only partially reversible, even after carpal tunnel surgery.
Thenar Atrophy
Thenar muscle atrophy indicates chronic denervation:
- Visible flattening or hollowing at the base of the thumb
- Weakness of abductor pollicis brevis and opponens pollicis on examination
- Often accompanied by reduced CMAP amplitude of the median nerve on EMG
Presence of thenar atrophy signals severe CTS and usually justifies prompt surgical treatment.
Loss of Grip Strength
Median nerve motor dysfunction and pain lead to:
- Decreased grip and pinch strength
- Difficulty lifting objects or performing twisting tasks (jars, bottle caps)
- Reduced endurance with repetitive manual work
Objective dynamometer measurements often lag behind subjective improvement after decompression and may continue to improve for months.
Nocturnal Numbness
Nocturnal numbness is often the first and most bothersome symptom:
- Occurs especially in the early morning hours
- Frequently bilateral, but may be asymmetric
- “Shaking out” the hands or dangling them off the bed gives transient relief
What Carpal Tunnel Feels Like (Sensory Description)
Patients commonly describe:
- Tingling, “pins and needles,” or “electric shocks” in thumb–index–middle–radial ring finger
- Burning or tightness in the palm
- Sensory changes sparing the little finger (critical for differential diagnosis)
- Occasionally, referred pain into the proximal forearm or even shoulder
Symptoms outside the median distribution (e.g., whole hand, neck, shoulder) are common but nonspecific; they do not exclude CTS but should prompt careful evaluation for additional pathologies (double crush, cervical radiculopathy, thoracic outlet).
Symptom Severity Table
| Severity Level | Sensory Symptoms | Motor Symptoms | Nocturnal Symptoms | Exam Findings (Typical) |
|---|---|---|---|---|
| Mild | Intermittent tingling, numbness in median digits; daytime mostly normal | None or subtle clumsiness | Frequent hand numbness at night; relieved by shaking | Normal strength; mildly decreased light touch or normal; provocative tests often positive |
| Moderate | Daily paresthesia; intermittent daytime numbness | Subjective weakness; dropping objects | Night symptoms most nights; may disturb sleep repeatedly | Decreased two-point discrimination; mild thenar weakness; abnormal sensory NCS |
| Severe | Constant numbness; may have pain or burning | Thenar atrophy; marked weakness of thumb abduction/opposition | Numbness often constant; night symptoms less prominent simply because sensation is lost | Absent or markedly impaired sensibility; thenar wasting; motor NCS/EMG shows denervation |
4. Causes and Risk Factors
CTS usually reflects a multifactorial interplay of local anatomy, systemic conditions, and occupational or biomechanical exposures. Many patients have no single identifiable cause.
Repetitive Wrist Motion
High-quality evidence links CTS to:
- High repetition and high force hand use
- Tasks above the ACGIH hand activity level
- High Strain Index workloads (HR ~1.6–1.9 vs low exposure)
Examples:
- Assembly line work
- Meat/poultry processing
- Industrial tool handling
In contrast, intensive computer keyboard use alone is not strongly associated with CTS and may even be associated with a lower rate of work-related CTS in some cohorts.
Pregnancy
Pregnancy can provoke transient CTS via:
- Hormonal changes (especially progesterone)
- Fluid retention and synovial edema
Symptoms typically arise in the third trimester and may remit postpartum, though some women develop persistent CTS requiring further management.
Diabetes Mellitus
Diabetes increases CTS risk through:
- Peripheral nerve susceptibility to ischemia
- Microvascular compromise
- Glycation of connective tissue
Diabetic patients may have more severe or bilateral CTS and may exhibit less complete recovery following decompression.
Hypothyroidism
Hypothyroidism can cause:
- Myxedematous thickening of perineurium and tendons
- Mucopolysaccharide deposition in the tunnel
Severe untreated hypothyroidism is a well-established risk factor; association with milder disease is less robust but commonly considered clinically.
Rheumatoid Arthritis (RA)
RA contributes via:
- Synovial hypertrophy around flexor tendons
- Tenosynovitis and joint deformity
- Occasional acute flares leading to acute carpal tunnel syndrome
CTS is a frequent hand manifestation in RA populations.
Obesity
Higher BMI is consistently associated with increased CTS risk, likely due to:
- Larger soft-tissue volumes
- Low-grade systemic inflammation
Weight reduction may modestly reduce symptom burden but is rarely a standalone solution.
Wrist Fracture and Trauma
- Distal radius fractures, carpal fractures, or dislocations can acutely narrow the tunnel or provoke hemorrhage and swelling.
- Post-traumatic deformity can cause chronic tunnel stenosis.
Acute CTS after trauma is a surgical emergency; chronic post-traumatic CTS follows usual principles but requires attention to bony alignment.
Genetic Predisposition
Familial clustering and anatomical variation (smaller carpal tunnel cross-sectional area) suggest genetic contributions:
- Some individuals have inherently narrower tunnels
- Connective tissue composition may predispose to SSCT fibrosis
Occupational Risk
Occupational risk factors with strongest evidence:
- High repetition + high force hand tasks
- Forceful gripping (>1 kgm force), especially without job rotation
- Use of certain hand-held vibrating tools (associations are mixed but acknowledged in some regulatory frameworks)
Computer use alone is a weak or negative risk factor; clinicians should avoid over-attributing CTS to typing without considering forceful, repetitive manual tasks.
Modifiable vs Non-Modifiable Risk Factors
Modifiable:
- High-force, high-repetition manual tasks
- Prolonged extremes of wrist flexion/extension
- Obesity
- Poor ergonomics (non-neutral wrist during tool or keyboard use)
- Smoking (potential small effect via microvascular mechanisms)
Non-modifiable (or partly modifiable):
- Age
- Female sex
- Smaller carpal tunnel anatomy
- Pregnancy (short-term modifiable)
- Underlying systemic disease (RA, diabetes, hypothyroidism—partly modifiable with treatment)
- Prior wrist fracture or deformity
5. Differential Diagnosis (OUTRANK SECTION)
CTS symptoms overlap with multiple disorders affecting the cervical roots, brachial plexus, peripheral nerves, and tendons. Misdiagnosis is common on patient forums and even in clinical practice. Careful mapping of symptom distribution, provocative maneuvers, and targeted testing is essential.
Key Conditions to Differentiate from CTS
Cubital Tunnel Syndrome (Ulnar Neuropathy at the Elbow)
- Nerve involved: Ulnar nerve at the elbow or ulnar groove
- Sensory pattern: Numbness/tingling of little finger and ulnar half of ring finger; often dorsoulnar hand involvement
- Motor pattern: Weakness of intrinsic hand muscles (interossei, adductor pollicis) with ulnar clawing; sparing of thenar abductor pollicis brevis
- Provocation: Elbow flexion, leaning on elbow, night symptoms with flexed elbow
Cervical Radiculopathy (C6–C8/T1)
- Nerve roots: Cervical roots compressed by disc herniation or spondylosis
- Sensory pattern: Dermatomal (may involve entire hand, forearm, and arm), often including dorsal hand and arm
- Pain: Neck pain and radiating arm pain; worsened by neck movements; Spurling’s test may reproduce symptoms
- Motor pattern: Weakness beyond median distribution (wrist extensors, triceps, etc.)
- Imaging/EMG: Cervical MRI or EMG localizing pathology proximally
Thoracic Outlet Syndrome (TOS)
- Site: Brachial plexus and/or subclavian vessels at thoracic outlet
- Symptoms: Diffuse paresthesia in entire arm/hand; aggravated by overhead or abducted arm positions
- Vascular signs: Possible discoloration, swelling, temperature changes; positive vascular maneuvers
- Imaging: Often normal; diagnosis relies heavily on clinical pattern, specialized imaging, and exclusion of other causes
Peripheral Neuropathy (e.g., Diabetic Polyneuropathy)
- Pattern: Length-dependent, symmetric, stocking-glove distribution
- Symptoms: Numbness, burning, and tingling in both feet before hands
- Course: Chronic, progressive; often coexists with CTS, complicating interpretation
- Tests: NCS/EMG show widespread sensory and sometimes motor involvement beyond median territory
Tendinitis and De Quervain’s Tenosynovitis
- De Quervain’s: Pain over radial styloid, worsened by thumb motion and ulnar deviation (positive Finkelstein test)
- Flexor or extensor tendinitis: Localized tendon pain; no true numbness or paresthesia
- Key distinction: Tendon conditions cause pain with motion and palpation but do not produce sensory loss in a nerve distribution.
Differential Diagnosis Comparison Table
| Condition | Primary Site | Sensory Pattern | Key Provocative Factors | Motor Findings | Diagnostic Clues |
|---|---|---|---|---|---|
| Carpal tunnel syndrome | Median nerve at wrist | Thumb, index, middle, radial ring; palm spared | Night, wrist flexion/extension, gripping | Thenar weakness/atrophy in severe CTS | Positive Phalen/Tinel/Durkan; median NCS abnormal |
| Cubital tunnel syndrome | Ulnar nerve at elbow | Little finger + ulnar ring; dorsoulnar hand | Elbow flexion, leaning on elbow | Intrinsic hand weakness; ulnar clawing | Tinel at elbow; ulnar NCS abnormal |
| Cervical radiculopathy | Cervical roots (C6–T1) | Dermatomal; often neck/arm pain too | Neck extension/rotation (Spurling) | Proximal muscle weakness (e.g., triceps, wrist extensors) | Cervical MRI/EMG localize root lesion |
| Thoracic outlet syndrome | Brachial plexus outlet | Diffuse arm/hand; sometimes whole hand | Overhead or abducted arm positions | Variable; may include intrinsic hand | Vascular signs, provocative TOS maneuvers |
| Peripheral neuropathy | Length-dependent nerves | Stocking-glove (feet before hands) | Not position-specific | Symmetric distal weakness in advanced disease | NCS show widespread symmetric involvement |
| De Quervain’s / tendinitis | Tendon sheaths | No true numbness; localized pain | Specific thumb/wrist movements | Normal strength (limited by pain) | Local tenderness; imaging if needed; normal NCS |
Clinically, double crush (e.g., cervical radiculopathy plus CTS) is not rare and may explain incomplete symptom resolution after isolated carpal tunnel surgery.
6. How Doctors Diagnose Carpal Tunnel Syndrome
Diagnosis integrates history, physical examination, and—when needed—confirmatory tests. AAOS and neurology guidelines emphasize that CTS is primarily a clinical diagnosis, with tests used to support uncertain cases, stage severity, or plan surgical treatment.
Physical Examination Tests
Key provocative maneuvers:
- Phalen’s test: Maximal wrist flexion for 30–60 seconds reproduces median paresthesia in CTS.
- Reverse Phalen: Wrist extension at same duration (less commonly used).
- Tinel’s sign at the wrist: Tapping over the carpal tunnel elicits tingling in median digits.
- Durkan (carpal compression) test: Direct manual compression over the carpal tunnel reproduces symptoms; often more sensitive than Tinel or Phalen.
Sensitivity and specificity of these tests vary widely across studies, and correlation with NCS findings is imperfect. A thorough sensory and motor exam of both median and ulnar territories, plus neck and proximal limb evaluation, is critical for proper differential diagnosis.
Nerve Conduction Study (NCS)
NCS evaluate:
- Distal sensory latency (DSL)
- Distal motor latency (DML)
- Conduction velocities and amplitudes across the carpal tunnel
Systematic review data indicate weighted mean sensitivity and specificity for:
Key points:
- Normal NCS does not exclude clinically mild CTS, especially early disease or intermittent symptoms.
- Abnormal NCS help confirm diagnosis, grade severity, and are often obtained before surgical treatment, particularly in atypical cases or when medicolegal issues exist.
Electromyography (EMG)
Needle EMG:
- Assesses motor unit recruitment and denervation in thenar muscles (abductor pollicis brevis)
- Helps distinguish CTS from more proximal lesions (cervical roots, plexus, proximal median neuropathy)
EMG is most useful when:
- Distribution of symptoms is atypical
- Differential diagnosis includes cervical radiculopathy, brachial plexopathy, or generalized neuropathy
- There is suspected severe axonal loss or long-standing weakness
Ultrasound
High-resolution ultrasound can directly visualize the median nerve:
- Measures cross-sectional area (CSA) at the tunnel inlet and proximally
- Assesses flattening, bowing of the flexor retinaculum, and SSCT changes
A systematic review/meta-analysis:
- Pooled sensitivity ~0.80 and specificity ~0.90 for CTS diagnosis using CSA thresholds
Other clinical trials show similar diagnostic accuracy and usefulness in staging severity and detecting structural anomalies.
Advantages:
- Non-invasive, painless, relatively low cost
- Provides anatomical information (e.g., tenosynovitis, ganglion, anomalous muscles)
Limitations:
- Operator-dependent
- Cut-off values vary across studies and populations
MRI (When Needed)
MRI is not routinely required but may be considered when:
- A mass lesion (tumor, ganglion, synovial cyst) is suspected
- Recurrent or persistent symptoms after surgery raise concern for incomplete release, scarring, or other pathology
- There is atypical presentation or suspicion of systemic amyloidosis or infiltrative diseases
False Positives and Limitations
- Up to 10–20% of asymptomatic individuals may have NCS abnormalities suggestive of CTS, especially in older or diabetic populations.
- Clinical tests have variable sensitivity and specificity and may not correlate tightly with electrodiagnostic findings.
- Overreliance on a single test (e.g., NCS alone or ultrasound alone) risks misclassification; integration of history, exam, and tests remains the standard.
- AAOS guidelines emphasize that routine preoperative NCS is not mandatory in classic, straightforward CTS but is often prudent in atypical or high-risk cases.
7. Severity Staging
Severity is typically graded clinically and electrodiagnostically:
- Mild CTS:
- Moderate CTS:
- Severe CTS:
Treatment Pathway by Stage
| Stage | Typical Clinical Picture | Preferred Initial Management |
|---|---|---|
| Mild | Intermittent nocturnal paresthesia, no weakness/atrophy | Night wrist splint, activity modification, short trial of non-surgical treatment; consider steroid injection in selected cases |
| Moderate | Daytime symptoms, functional impact, early weakness | Non-surgical measures; consider earlier move to surgery if symptoms persist beyond several weeks–months or significantly affect work/sleep |
| Severe | Constant numbness, thenar atrophy, marked weakness | Prompt surgical decompression (open or endoscopic) to prevent further irreversible nerve damage |
AAOS and other guidelines support trying non-operative treatment in mild–moderate CTS, but recognize that severe CTS with denervation is best managed with timely surgery.
8. Non-Surgical Treatment
Non-surgical (conservative) options are mainly appropriate for mild to moderate CTS and for transient CTS (e.g., pregnancy-related). Evidence quality varies; some popular treatments lack strong support.
Wrist Splints
Neutral-position wrist splints:
- Reduce extremes of flexion/extension, lowering intracarpal pressure
- Are particularly effective for nocturnal symptoms
Evidence:
- Cochrane and subsequent reviews show low- to moderate-certainty evidence that night splinting improves symptoms in mild–moderate CTS vs no treatment over the short term.
- Continuous wear (day + night) is not clearly superior to night-only and is less tolerated.
Clinical use:
- First-line in early CTS
- Often combined with activity modification and ergonomic interventions
NSAIDs
Nonsteroidal anti-inflammatory drugs:
- May reduce pain related to concomitant tendinitis or synovitis
- Do not address the primary mechanism of median nerve compression
Evidence:
NSAIDs should be viewed as symptomatic adjuncts, not disease-modifying CTS therapy.
Corticosteroid Injections
Local corticosteroid injections into or proximal to the carpal tunnel:
- Temporarily reduce synovial inflammation and edema
- Provide symptom relief in many patients for weeks to months
Evidence:
- Randomized trials and Cochrane reviews show moderate-certainty evidence of short-term (up to 3 months) symptom improvement vs placebo.
- Effect often wanes; many patients ultimately proceed to surgery.
Risks:
- Transient nerve irritation, local pain
- Rare tendon rupture or intraneural injection
Guideline trend (AAOS 2024 update):
- Corticosteroid injections are optional, not mandatory, and should be weighed against the goal of definitive decompression in patients with significant or progressive symptoms.
Activity Modification
Key elements:
- Avoid prolonged wrist flexion/extension and forceful gripping where possible
- Alter tools, work cycles, and job rotation in high-strain workplaces
- Reduce or reconfigure tasks involving vibrating tools
Evidence from occupational studies supports that reducing high force + high repetition exposure decreases CTS incidence and severity.
Ergonomic Correction
Effective ergonomic measures:
- Maintain neutral wrist posture at keyboards and with hand tools
- Adjust chair, desk, and mouse to avoid wrist extension or ulnar deviation
- Use padded supports judiciously (avoiding direct, rigid pressure on the carpal tunnel)
Cochrane reviews of ergonomic interventions show mixed evidence; benefits are more plausible in high-risk manual occupations than in office-only work.
Nerve Gliding Exercises
Median nerve and tendon gliding exercises are widely prescribed:
- Aim to promote nerve mobility within the tunnel and reduce adhesions
- Protocols combine sequences of wrist, finger, and elbow positions
Evidence:
- Some small studies suggest short-term symptom improvement, but data quality is low and effect size modest.
- Should be considered adjunctive, not standalone treatment.
Physical Therapy
Physical/occupational therapy modalities may include:
- Education and ergonomic training
- Manual therapy
- Ultrasound therapy
- Stretching and strengthening
Overall, evidence is heterogeneous:
- No strong, consistent benefit over splinting alone for most modalities
- May add value for coexisting musculoskeletal issues (neck, shoulder, forearm) but do not reverse structural median nerve compression.
What Works vs What Lacks Strong Evidence
Supported by moderate or better evidence:
- Night wrist splints (particularly for mild–moderate CTS)
- Local corticosteroid injection for short-term relief
- Surgical treatment vs splinting for sustained improvement at 6–12 months in suitable candidates
Limited or inconsistent evidence:
- Oral NSAIDs and systemic steroids as primary CTS therapy
- Therapeutic ultrasound, laser, acupuncture, PRP, shockwave therapy
- Vitamins, supplements, “nerve vitamins,” and most alternative treatments
Patients should be counseled that non-surgical treatment may alleviate symptoms but is less likely to produce durable resolution when significant structural compression is present.
9. Surgical Treatment
When Surgery Is Necessary
Indications for carpal tunnel surgery (carpal tunnel release) include:
- Severe CTS:
- Constant numbness
- Thenar atrophy or clear weakness
- EMG evidence of denervation
- Failure of adequate non-surgical treatment (e.g., splinting and/or injection) over several weeks–months
- Significant functional impairment (work, daily activities) despite conservative measures
- Acute CTS (e.g., after fracture, hematoma, or severe inflammatory flare) with rapidly progressive deficits (emergent decompression)
Surgery aims to decompress the median nerve by dividing the transverse carpal ligament.
Open Carpal Tunnel Release (Open Release)
Technique (standard open release):
- Small longitudinal or curvilinear incision over the palm, just ulnar to the thenar crease
- Direct visualization of the transverse carpal ligament and median nerve
- Complete division of the ligament from distal to proximal
- Inspection for anomalous structures or masses
- Wound closure; ligament is not reconstructed
Advantages:
- Direct visualization of anatomy
- Familiar to most surgeons
- Versatile in revision and complex cases
Disadvantages:
- Larger skin incision vs endoscopic
- Pillar pain (tenderness at thenar/hypothenar pillars) and scar sensitivity in some patients
- Potentially longer time to return to heavy manual work compared with endoscopic techniques
Endoscopic Carpal Tunnel Release (Endoscopic Release)
Technique (single- or dual-portal):
- One or two small incisions in distal forearm/palm
- Endoscope inserted under the transverse carpal ligament
- Division of the ligament under endoscopic visualization
Advantages (from meta-analyses and RCTs):
- Faster early symptom relief and functional recovery
- Less scar tenderness and pillar pain
- Earlier return to work in many series
Disadvantages:
- Steeper learning curve
- Slightly higher risk of iatrogenic nerve or vessel injury in some early series (though modern large datasets show comparable nerve injury rates)
- Higher direct procedural cost in many systems
Recovery Timeline
Typical (non-emergent) recovery after uncomplicated release:
- Immediate postoperative (days 1–7):
- Soft dressing; early finger motion encouraged
- Mild to moderate pain at incision and palm
- Weeks 1–3:
- Sutures removed ~10–14 days
- Light activities of daily living as tolerated
- Many patients resume light keyboard use within 1–2 weeks, depending on pain and job demands
- Weeks 4–6:
- Months 3–12:
These ranges are general; individual recovery varies widely.
Complications
Potential complications of carpal tunnel surgery:
- Common but usually transient:
- Pillar pain (ache at thenar/hypothenar pillars)
- Incisional tenderness or scar sensitivity
- Temporary flare of neuropathic symptoms
- Less common:
- Wound infection
- Hematoma
- Complex regional pain syndrome (rare)
- Serious but rare:
Large database and meta-analytic data indicate overall complication rates are low and similar between open and endoscopic approaches, though patterns differ (e.g., more wound issues with open, higher cost with endoscopic).
Recurrence Rate and Revision Surgery
“Recurrence” must be distinguished from:
- Persistent symptoms due to incomplete initial release
- Progression of proximal pathology (e.g., cervical radiculopathy, diabetic neuropathy)
Published series vary, but:
- Most report good to excellent symptom relief in 70–90% of patients
- Clinically significant persistent or recurrent CTS necessitating revision surgery is seen in roughly 5–10%, depending on population and definition
Common causes of failed primary surgery:
- Incomplete ligament division
- Perineural scarring and adhesions
- Unrecognized double crush or concomitant neuropathy
- Underlying systemic conditions (e.g., amyloidosis, diabetes) limiting nerve recovery
Revision surgery often involves extended open exposure, neurolysis, and careful exploration; outcomes are generally less predictable than primary release.
Success Statistics
Systematic reviews and large cohort analyses show:
- High rates of symptom improvement and patient satisfaction after both open and endoscopic carpal tunnel release
- No consistent difference in long-term symptom relief between approaches
- Endoscopic release often shows:
Open vs Endoscopic: Comparison Table
Choice of approach should consider surgeon expertise, patient anatomy and comorbidities, job demands, and local resource factors. There is no single “best” technique for all patients.
10. Recovery Timeline
Post-Surgery Expectations
- Numbness and tingling often improve quickly, sometimes immediately; in chronic severe CTS, improvement may be slower and incomplete.
- Pain from the incision and pillar region usually subsides over weeks.
- Swelling and stiffness may persist for several weeks; early finger motion is encouraged.
Return to Typing
For many office workers:
- Light typing may resume within 1–2 weeks, depending on pain and wound healing.
- Full comfort and endurance at the keyboard may take several weeks.
- Neutral wrist positioning and ergonomic adjustments are important to avoid overuse of the healing tissues.
Return to Manual Labor
For heavy manual workers:
- Light duties may be possible at ~3–4 weeks.
- Full-duty heavy lifting, repetitive force tasks, or vibrating tool use often postponed until 6–8+ weeks, tailored to recovery and job demands.
Endoscopic release may allow somewhat earlier return to full work, but patient- and job-specific factors dominate decisions.
Full Nerve Recovery Duration and Nerve Regeneration Speed
Peripheral nerve recovery follows:
- Remyelination (for demyelinating lesions): Often within weeks–months after decompression
- Axonal regeneration (for axonal loss): Commonly cited rates are approximately 1 mm/day along the nerve; functional recovery depends on distance to target and central adaptation
For CTS:
- Sensory improvement may continue for 6–12 months or longer
- Motor recovery (thenar bulk and strength) may continue up to 1–2 years but can remain incomplete in long-standing severe CTS
Patients should be counseled that:
- Early symptom changes do not fully predict long-term outcome
- Persistent deficits months after surgery reflect preoperative nerve damage as much as surgical efficacy
11. Can Carpal Tunnel Syndrome Heal on Its Own?
Natural history data suggest:
- Some mild CTS cases—especially those related to pregnancy or reversible exposures—can partially or completely remit without surgery.
- However, many cases either remain stable or slowly worsen over time if compression persists; progression to constant numbness and thenar atrophy is associated with permanent deficits even after later decompression.
Factors favoring non-operative resolution:
- Short symptom duration
- Mild, intermittent symptoms
- Reversible triggers (pregnancy, short-term overload)
- Absence of thenar weakness or denervation on EMG
In contrast, relying on spontaneous recovery in moderate–severe CTS with objective deficits risks irreversible nerve damage. Management decisions should be individualized in consultation with a qualified clinician.
12. Prevention Strategies
Ergonomics
Key ergonomic measures for CTS risk reduction:
- Maintain neutral wrist posture during tasks (keyboards, tools, musical instruments)
- Avoid prolonged extreme flexion or extension
- Minimize forceful gripping and pinching when possible
- Break up highly repetitive or forceful tasks with rest or task variation
Workplace interventions should prioritize lowering the combination of force + repetition, which has the strongest evidence for work-related CTS risk.
Keyboard Positioning
For computer users:
- Keyboard at or slightly below elbow height
- Wrists straight, not resting on hard edges
- Mouse close to the body, with minimal wrist deviation
- Use software or work routines encouraging brief microbreaks
High computer use alone is not a major independent cause of CTS, but poor posture can aggravate symptoms in susceptible individuals.
Stretching Myths
Simple stretching alone:
- Does not reverse structural median nerve compression
- May improve comfort transiently in mild symptoms or coexisting tendon issues
Nerve gliding and stretching should be framed as adjuncts, not as stand-alone curative treatments. Overemphasis on stretching as a “cure” is a common misconception on non-medical forums.
Workplace Modification
Effective strategies for at-risk occupations:
- Task redesign to reduce high-force, high-repetition cycles
- Job rotation to reduce unilateral overuse
- Tool redesign (e.g., power tools with lower required grip force, improved handle design)
- Control of hand-arm vibration exposures where relevant
Occupational medicine input is valuable for workers with recurrent or bilateral CTS.
13. Living With Carpal Tunnel Syndrome
Sleep Positioning
To reduce nocturnal symptoms:
- Avoid sleeping with wrists flexed or hands under pillows
- Use a neutral-position wrist splint at night if tolerated
- Try side-lying positions with arms supported by pillows to avoid prolonged wrist flexion/extension
These measures can significantly reduce hand numbness at night in mild–moderate CTS.
Daily Coping Strategies
- Schedule symptom-provoking tasks earlier in the day when possible
- Use adaptive equipment (jar openers, larger handles) to reduce grip force demands
- Plan regular microbreaks with gentle finger and wrist range-of-motion
- Manage systemic risk factors (glucose control, thyroid replacement, weight management, RA control)
Patients with progressive functional loss should not rely solely on coping strategies; definitive evaluation for surgical treatment should be considered.
When to Seek Urgent Care
Urgent or emergent evaluation is warranted if:
- Sudden severe pain, swelling, and rapidly progressive numbness/weakness occur after trauma (possible acute CTS requiring emergent decompression)
- New profound hand weakness or inability to move the thumb develops over hours to days
- Symptoms are accompanied by systemic signs (fever, severe redness, suspected infection)
Non-emergent but prompt evaluation is appropriate when:
- Symptoms have persisted beyond a few weeks and impair work or daily function
- Numbness is constant or thenar atrophy is noticed
- There is diagnostic uncertainty (neck, shoulder, or other nerve symptoms)
14. Frequently Asked Questions (Schema Ready)
Q1. How do I know if I have carpal tunnel syndrome?
CTS typically causes tingling, numbness, or burning in the thumb, index, middle, and radial half of the ring finger, often worse at night or with activities like driving or holding a phone. The little finger is usually spared. Shaking the hand often brings temporary relief. Over time, you may notice dropping objects, reduced dexterity, or weakness at the base of the thumb. A clinician confirms the diagnosis based on symptom pattern, physical examination, and sometimes nerve conduction studies or ultrasound. Similar symptoms can arise from the neck, elbow, or generalized neuropathy, so self-diagnosis is unreliable.
Q2. Is carpal tunnel usually treated without surgery?
Mild to moderate CTS is often managed initially without surgery. Common non-surgical treatments include night wrist splints, activity and ergonomic modification, and sometimes local corticosteroid injections. These approaches can significantly reduce symptoms, especially when disease is early or associated with transient factors such as pregnancy. However, if symptoms persist, worsen, or are associated with constant numbness or muscle wasting, surgery is usually recommended. Non-surgical treatment is less effective once there is clear nerve damage (thenar atrophy, marked weakness, severe electrodiagnostic changes).
Q3. What is the most effective treatment for carpal tunnel syndrome?
For persistent, clinically significant CTS, surgical decompression (carpal tunnel release) is the most effective long-term treatment. High-quality evidence shows surgery provides greater and more durable symptom improvement than splinting alone at 6–12 months. Non-surgical options—splints, injections, and activity modification—are valuable for mild disease, short-term relief, or when surgery must be delayed. In severe CTS with constant numbness, thenar atrophy, or significant nerve conduction abnormalities, prompt surgery offers the best chance to prevent further permanent nerve damage. The choice depends on symptom severity, duration, comorbidities, and patient goals.
Q4. Can carpal tunnel syndrome cause permanent damage?
Yes. Prolonged median nerve compression can progress from reversible demyelination to axonal loss. Once axons are lost and thenar muscles are chronically denervated, recovery becomes incomplete even after surgical decompression. Clinically, constant numbness, markedly reduced sensibility, and visible thenar muscle atrophy suggest advanced neuropathy. Surgery can still prevent further deterioration and may yield partial improvement, but full restoration of normal sensation and strength is less likely. Early recognition and timely treatment—especially before constant numbness and atrophy—substantially reduce the risk of permanent deficits.
Q5. How long does carpal tunnel surgery take?
Carpal tunnel release is usually a short outpatient procedure. In straightforward cases, operative time is often 10–30 minutes per hand, depending on technique and surgeon. Patients typically go home the same day. The total time at the facility is longer due to preoperative preparation, anesthesia, and postoperative observation. Stitches are usually removed around 10–14 days after surgery. Although the operation itself is brief, full functional recovery can take weeks to months, particularly for heavy manual work or in severe long-standing disease.
Q6. Can carpal tunnel syndrome come back after surgery?
True recurrence after a complete and properly performed release is uncommon but possible. More often, patients experience persistent symptoms from incomplete initial decompression or from additional problems such as cervical radiculopathy, ulnar neuropathy, or diabetic polyneuropathy. Scar tissue around the nerve can also contribute to recurrent symptoms. Reported rates of clinically significant recurrence or persistent CTS requiring revision surgery are generally in the single-digit to low double-digit percentages, depending on population and definition. Proper evaluation of persistent or recurrent symptoms should include reassessment of the entire nerve pathway, not just the wrist.
Q7. Is typing the main cause of carpal tunnel syndrome?
Contrary to popular belief, high-quality epidemiologic studies do not support typical computer keyboard use as a major independent cause of CTS. The strongest occupational risks are tasks involving both high repetition and high force, particularly in industrial and manual labor settings. Hand-arm vibration and forceful gripping also contribute in some jobs. Poor keyboard ergonomics can aggravate symptoms in susceptible individuals, but many patients with CTS have minimal computer use. It is more accurate to consider typing as a potential aggravating factor rather than the primary cause in most cases.
Q8. Does carpal tunnel syndrome affect the whole hand?
Classic CTS affects the thumb, index, middle, and radial half of the ring finger—areas supplied by the median nerve. The little finger is usually unaffected, and the central palm often remains normal because its sensory branch travels outside the carpal tunnel. However, many patients subjectively report “whole hand” discomfort or aching, especially early on. True numbness involving the little finger or the back of the hand suggests additional or alternative diagnoses such as ulnar neuropathy, cervical radiculopathy, or more generalized neuropathy.
Q9. How long does it take to recover from carpal tunnel surgery?
Most patients notice improvement in tingling and numbness within days to weeks. Light activities and desk work often resume within 1–2 weeks, while heavy manual work may require 4–8 or more weeks depending on job demands and individual recovery. Grip strength and fine dexterity can continue to improve for several months. In severe, long-standing CTS, full recovery of sensation and strength may take up to a year or more and may remain incomplete. Postoperative course should be individualized with your surgeon.
Q10. Can I treat carpal tunnel syndrome at home?
Early or mild CTS symptoms can sometimes be managed at home with night wrist splints, ergonomic adjustments, and activity modification. Avoiding prolonged wrist flexion or extension and reducing high-force repetitive tasks can help. However, home treatment should not replace professional evaluation when: symptoms persist beyond a few weeks, interfere with sleep or work, become constant, or are associated with weakness or visible muscle wasting. Self-treatment without proper diagnosis risks missing alternative or more serious conditions.
Q11. Do I need a nerve conduction study before surgery?
Not always. In classic, straightforward CTS with typical symptoms and exam findings, some guidelines allow surgery without mandatory nerve conduction studies. However, many surgeons still obtain NCS (and sometimes EMG) before surgery to confirm diagnosis, grade severity, and document baseline status—especially when symptoms are atypical, bilateral, or legally sensitive. NCS are also valuable to identify additional neuropathies or proximal lesions. The decision should be made jointly with your treating clinician, based on your clinical scenario and local standards.
Q12. Can carpal tunnel syndrome be cured without surgery?
In some patients with mild, early CTS—particularly when related to pregnancy or a reversible occupational exposure—symptoms can resolve with non-surgical measures alone. Night splints, ergonomic changes, and occasionally corticosteroid injections may yield durable relief. However, in many others, these measures only control symptoms temporarily. Once structural compression is significant or nerve damage has occurred, surgery is usually the only way to reliably decompress the nerve. There is no guaranteed “cure” in all cases, but appropriate treatment can substantially reduce symptoms and prevent progression.
Q13. Is carpal tunnel syndrome dangerous?
CTS is rarely life-threatening, but it can be functionally disabling and may cause permanent nerve damage if ignored. Advanced CTS can lead to constant numbness, chronic pain, and loss of thumb function, significantly impairing work and daily activities. In the specific context of acute CTS after trauma or infection, rapid progression of symptoms is an emergency requiring prompt decompression to prevent irreversible deficits. Seeking appropriate evaluation and timely treatment is important to avoid long-term disability.
15. Key Clinical Takeaways
- Carpal tunnel syndrome is the most common entrapment neuropathy, caused by median nerve compression within a rigid osteofibrous canal at the wrist.
- Pathophysiology involves raised intracarpal pressure, microvascular ischemia, demyelination, and, in chronic cases, axonal degeneration and SSCT fibrosis.
- Classic symptoms: nocturnal paresthesia in median digits, sparing the little finger, with progression to daytime symptoms, sensory loss, and thenar atrophy if untreated.
- Differential diagnosis must distinguish CTS from cubital tunnel syndrome, cervical radiculopathy, thoracic outlet syndrome, peripheral neuropathy, and tendon disorders; symptom mapping and targeted testing are crucial.
- Diagnosis is primarily clinical, supported as needed by nerve conduction studies, EMG, and ultrasound; no single test is perfectly sensitive or specific.
- Non-surgical treatment (night wrist splints, ergonomic modification, and sometimes corticosteroid injections) is appropriate for mild–moderate disease and short-term relief but less effective in severe neuropathy.
- Surgical decompression (open or endoscopic release) provides the most reliable long-term improvement, especially when symptoms are persistent, severe, or associated with objective deficits.
- Open and endoscopic carpal tunnel surgery have similar long-term outcomes; endoscopic techniques may offer faster early recovery but at higher cost and with a learning curve.
- Nerve recovery can continue for many months; advanced, long-standing CTS may leave residual deficits despite technically adequate decompression.
- High-force, high-repetition manual tasks and certain systemic conditions (diabetes, RA, hypothyroidism, obesity, pregnancy) are key risk factors; heavy keyboard use alone is a relatively minor contributor.
16. Medical Disclaimer
This article is for educational and informational purposes only. It does not provide medical diagnosis, individualized treatment recommendations, or professional medical advice. Carpal tunnel syndrome and its mimics can only be accurately evaluated by a qualified healthcare professional who has access to your full history, examination, and appropriate diagnostic tests.
Do not ignore new or worsening symptoms of hand numbness, weakness, or pain, and do not delay seeking medical care because of something you read here. For any questions about your own symptoms, risk factors, test results, or treatment options—including the need for surgery—consult a licensed physician (such as a neurologist, hand surgeon, or primary care clinician) in your jurisdiction. If you experience sudden severe pain, rapid weakness, or signs of infection or trauma, seek urgent or emergency medical attention.