1. What Is Carpal Tunnel Syndrome?
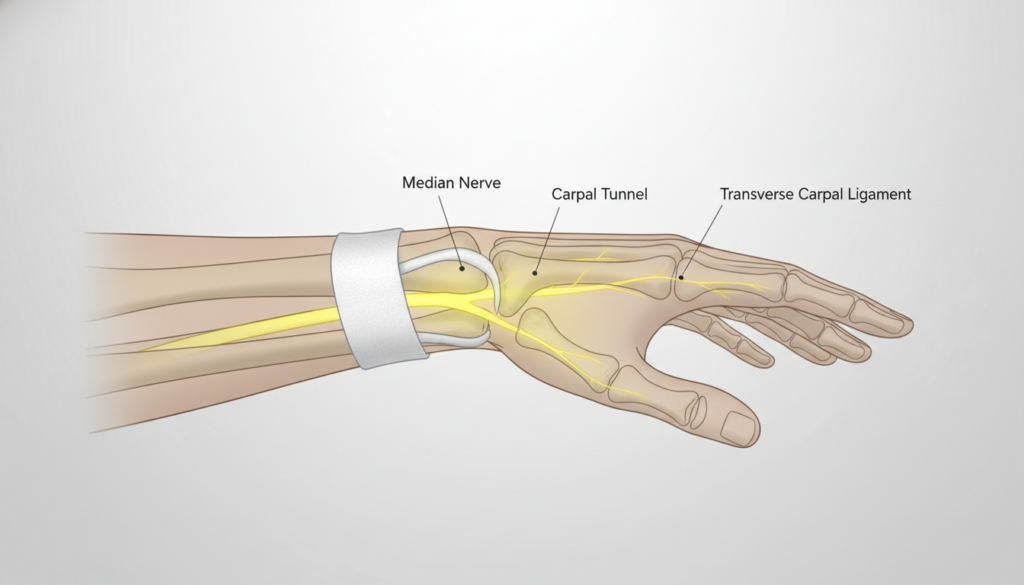
Carpal tunnel syndrome is a compressive neuropathy of the median nerve at the wrist. The median nerve travels from the neck down the arm and enters the hand through a narrow passageway called the carpal tunnel, formed by wrist bones (carpal bones) and the transverse carpal ligament.
When pressure increases within this confined space, the median nerve becomes compressed. Because this nerve supplies sensation to the thumb, index finger, middle finger, and part of the ring finger—and controls several thumb muscles—symptoms reflect both sensory and motor dysfunction.
Why Symptoms Develop Gradually
The median nerve does not fail abruptly in most cases. Instead:
- Repetitive stress, fluid retention, inflammation, or structural narrowing increases tunnel pressure.
- Venous outflow from the nerve becomes impaired.
- Nerve conduction slows due to ischemia and demyelination.
- Persistent compression eventually leads to axonal injury.
This progressive cascade explains why carpal tunnel symptoms often begin subtly and worsen over time. Early recognition is critical because nerve compression is far more reversible in the initial stages.
2. The Early Warning Signs of Carpal Tunnel
The early warning signs of carpal tunnel syndrome are often sensory and intermittent. Many patients dismiss them as temporary “hand fatigue.”
Common Early Symptoms
- Nighttime numbness
- Tingling in the thumb, index, and middle fingers
- “Hand falling asleep” sensation
- Mild grip weakness
- Symptoms that improve by shaking the hand
These warning signs reflect transient median nerve compression that becomes worse when the wrist is flexed or extended for prolonged periods—especially during sleep.
Why Nighttime Symptoms Occur
During sleep:
- Wrists often flex unconsciously.
- Fluid redistributes into extremities.
- Carpal tunnel pressure increases.
Median nerve perfusion decreases, leading to paresthesias (abnormal sensations).
Why Shaking the Hand Helps
Shaking the hand briefly:
- Reduces wrist flexion
- Improves venous return
- Temporarily lowers pressure inside the tunnel
This classic “flick sign” is strongly associated with early carpal tunnel syndrome.
Early Symptom Mechanism Table
| Early Symptom | Underlying Mechanism |
|---|---|
| Nighttime numbness | Increased tunnel pressure during wrist flexion and fluid shifts |
| Tingling in thumb/index/middle | Median nerve sensory fiber ischemia |
| Hand “falling asleep” | Transient nerve conduction block |
| Mild grip weakness | Early motor fiber involvement |
| Relief with shaking | Temporary decompression and improved perfusion |
At this stage, damage is typically demyelinating rather than axonal, meaning it is often reversible.
3. What Does Early Stage Carpal Tunnel Feel Like?
Patients describe early stage carpal tunnel in vivid sensory terms:
- “Pins and needles”
- Burning sensation
- Electric shock–like jolts
- Intermittent numbness
- Clumsiness when buttoning clothes
Symptoms often come and go. They may appear after typing, driving, or holding a phone.
The Sensory Pattern Matters
Carpal tunnel symptoms classically involve:
- Thumb
- Index finger
- Middle finger
- Radial half of ring finger
The small finger is spared because it is innervated by the ulnar nerve.
Addressing a Common Fear: “Could This Be ALS?”
Many individuals encountering hand weakness worry about amyotrophic lateral sclerosis (ALS).
Why ALS differs:
- ALS does not cause sensory symptoms like tingling or numbness.
- ALS weakness is progressive and not position-dependent.
- ALS does not improve by shaking the hand.
- ALS typically affects multiple muscle groups, not isolated median nerve distribution.
In contrast, carpal tunnel syndrome is a localized compressive neuropathy with sensory predominance in early stages.
4. Stages of Carpal Tunnel Syndrome (4-Level Model)
Carpal tunnel syndrome progresses along a spectrum. Not all patients reach advanced stages.
Stage 1 – Intermittent / Early
- Nighttime numbness
- Intermittent tingling
- No permanent sensory loss
- Normal muscle bulk
Reversible with conservative care.
Stage 2 – Persistent Sensory Changes
- Daytime numbness
- Reduced light touch sensation
- Frequent paresthesias
- Sleep disruption
Demyelination more sustained; still largely reversible.
Stage 3 – Motor Weakness
- Reduced grip strength
- Difficulty opening jars
- Thumb weakness (abduction)
- Dropping objects
Motor fibers increasingly affected.
Stage 4 – Advanced / Muscle Atrophy
- Thenar muscle wasting
- Constant numbness
- Loss of fine motor control
- Possible permanent nerve damage
Axonal loss occurs. Recovery becomes incomplete if prolonged.
Progression Table
| Stage | Symptoms | Nerve Damage | Reversible? | Treatment Approach |
|---|---|---|---|---|
| 1 | Intermittent paresthesia | Demyelination | Yes | Splinting, ergonomic changes |
| 2 | Persistent numbness | Sustained demyelination | Often | Splints, steroid injection |
| 3 | Motor weakness | Early axonal loss | Partially | Consider surgical decompression |
| 4 | Muscle atrophy | Significant axonal degeneration | Limited | Surgery to prevent further loss |
5. When Symptoms Become Serious
Certain findings suggest more advanced nerve compromise:
- Constant numbness
- Thenar muscle wasting
- Loss of thumb opposition
- Frequent dropping of objects
Irreversible Damage Threshold
If compression leads to prolonged axonal degeneration, reinnervation becomes incomplete. Nerve fibers regenerate at approximately 1 mm per day. Chronic severe compression may result in:
- Permanent sensory loss
- Persistent weakness
- Incomplete muscle recovery
Timely intervention prevents progression beyond reversible stages.
6. Conditions Often Mistaken for Carpal Tunnel
Several disorders mimic carpal tunnel syndrome. Distinguishing them is essential.
Arthritis
- Pain localized to joints
- Swelling and stiffness
- Not confined to median nerve distribution
Diabetic Neuropathy
- Symmetric numbness
- Involves both feet and hands
- Stocking-glove pattern
Cervical Radiculopathy
- Neck pain radiating to arm
- Dermatomal pattern
- May involve entire hand
Cubital Tunnel Syndrome
- Ulnar nerve compression at elbow
- Affects ring and small finger
- Worse with elbow flexion
Thoracic Outlet Syndrome
- Arm heaviness
- Vascular symptoms
- Diffuse hand involvement
Differential Diagnosis Table
| Condition | Numbness Distribution | Pain Location | Night Symptoms | Muscle Involvement |
|---|---|---|---|---|
| Carpal tunnel | Thumb, index, middle | Wrist/palm | Common | Thenar weakness |
| Arthritis | Joint-specific | Joints | Variable | Minimal |
| Diabetic neuropathy | Symmetric hands/feet | Diffuse | Less positional | Late-stage |
| Cervical radiculopathy | Dermatomal | Neck to arm | Variable | Myotomal |
| Cubital tunnel | Ring/small finger | Elbow | With elbow flexion | Interossei weakness |
This differentiation is critical for accurate tunnel treatment planning.
7. Who Is Most at Risk?
Modifiable Risk Factors
- Repetitive wrist flexion/extension
- Prolonged keyboard use
- Vibrating tools
- Poor ergonomics
- Obesity
Non-Modifiable Risk Factors
- Female sex
- Pregnancy
- Diabetes
- Hypothyroidism
- Rheumatoid arthritis
- Genetic wrist anatomy
Pregnancy-related tunnel syndrome is often temporary due to fluid retention.
8. When to See a Doctor
Medical evaluation is recommended if:
- Symptoms last more than two weeks
- Night symptoms occur daily
- Grip weakness develops
- Objects are frequently dropped
- Visible muscle wasting appears
Nerve conduction studies can confirm diagnosis and quantify severity.
9. Early Treatment Options
Treatment depends on stage.
Stage 1–2
- Neutral wrist splints (especially at night)
- Activity modification
- Ergonomic adjustments
- Physical therapy
- Short course corticosteroid injection
These are effective early carpal tunnel treatment strategies.
Stage 3–4
- Surgical decompression (carpal tunnel release)
- Consideration after failed conservative care
Evidence shows that early intervention improves outcomes. Among available treatment options, splinting has strongest evidence for mild disease, while surgery has highest long-term success in moderate-to-severe cases.
10. Can Early Carpal Tunnel Be Reversed?
Yes—early carpal tunnel can often be reversed if compression is relieved before axonal damage occurs.
Recovery Timeline
- Symptom improvement: Days to weeks
- Nerve remyelination: Weeks
- Functional recovery: Several weeks to months
If axonal loss has occurred, recovery may take months and may not be complete.
11. Frequently Asked Questions
How do I know if I have carpal tunnel?
Classic symptoms include nighttime numbness, tingling in the thumb/index/middle fingers, and relief with shaking the hand. Confirmation requires clinical examination and often nerve conduction testing.
What are the first signs?
The first signs are usually intermittent tingling and nighttime numbness affecting the median nerve distribution.
Can carpal tunnel go away on its own?
Mild cases, especially pregnancy-related tunnel syndrome, may resolve. Persistent symptoms generally require intervention.
Is it always painful?
No. Many patients experience numbness or tingling without significant pain.
Does pregnancy-related tunnel syndrome resolve?
Often yes. Symptoms typically improve postpartum as fluid retention decreases.
How fast does it progress?
Progression varies. Some cases remain mild for years; others worsen over months if untreated.
Is numbness permanent?
Numbness may become permanent if severe compression leads to prolonged axonal damage.
12. Key Takeaways
- Carpal tunnel syndrome is a median nerve compression at the wrist.
- Early warning signs include nighttime numbness and tingling.
- Symptoms often improve with shaking in early stages.
- Sensory symptoms precede weakness.
- Four stages range from intermittent paresthesias to muscle atrophy.
- Early treatment improves reversibility.
- Persistent weakness or muscle wasting requires prompt evaluation.
- Not all hand numbness is carpal tunnel—differential diagnosis matters.
13. Medical Disclaimer
This educational content is intended for informational purposes only and does not constitute medical advice. It does not replace clinical evaluation, diagnosis, or individualized treatment by a licensed healthcare professional. If you experience persistent numbness, weakness, or hand dysfunction, consult a qualified medical provider for appropriate assessment and care.